 It’s that time of the year again! MIPS data submission season is upon us.
It’s that time of the year again! MIPS data submission season is upon us.
Despite there being a partial federal government shutdown, the Centers for Medicare & Medicaid Services (CMS) is open and ready to receive Merit-based Incentive Payment System (MIPS) data from eligible clinicians who participated in Year 2 (2018) of the Quality Payment Program (QPP).
Clinicians must attest by April 2, 2019 at 8 P.M. EDT to avoid a -5% payment adjustment in 2020!
Decisions, decisions!
Submitting your data may be as complicated as the MIPS program itself! There are so many decisions to make and things to do before you are ready to attest.
If you don’t believe me, these are just a few high-level questions you should be asking yourself:
- Do I need to submit MIPS data?
- Are you excluded?
- Are you considered a Qualifying Participant (QP) in an Advanced Alternative Payment Model (AAPM)?
- Are you a part of a MIPS Alternative Payment Model (APM) that will submit data on your behalf?
- Am I submitting as an individual or a group?
- If you report MIPS data in as an individual, your payment adjustment will be based only on your performance. An individual is defined as a single National Provider Identifier (NPI) tied to a single Taxpayer Identification Number (TIN).
- If you report MIPS data as a group, your payment adjustment is based on the group’s A group is defined as a set of clinicians—identified by their NPI—sharing a common TIN, no matter the specialty or practice site. Keep in mind, if you are individually excluded, and yet your TIN is submitting MIPS data as a group, you will no longer be excluded and will need to submit MIPS data as part of the group submission. This is a decision to think carefully about.
Okay, let’s pause the list here. A quick way to see if you need to submit MIPS data is via the QPP participation lookup tool. This will display all entities associated with your NPI during the 2018 year. This lookup tool will also show if you are deemed a Qualifying Participant (QP)—allowing you to skip MIPS—or if you are associated with a MIPS APM.
It is important to remember that your eligibility in MIPS is on a TIN/NPI combination level. For example, if you belong to two different practices, or if you are in a practice and a MIPS APM, you will have to submit MIPS for every TIN/NPI combination in which you are MIPS-eligible.
Alright, carrying on…
- What MIPS reporting period will I select?
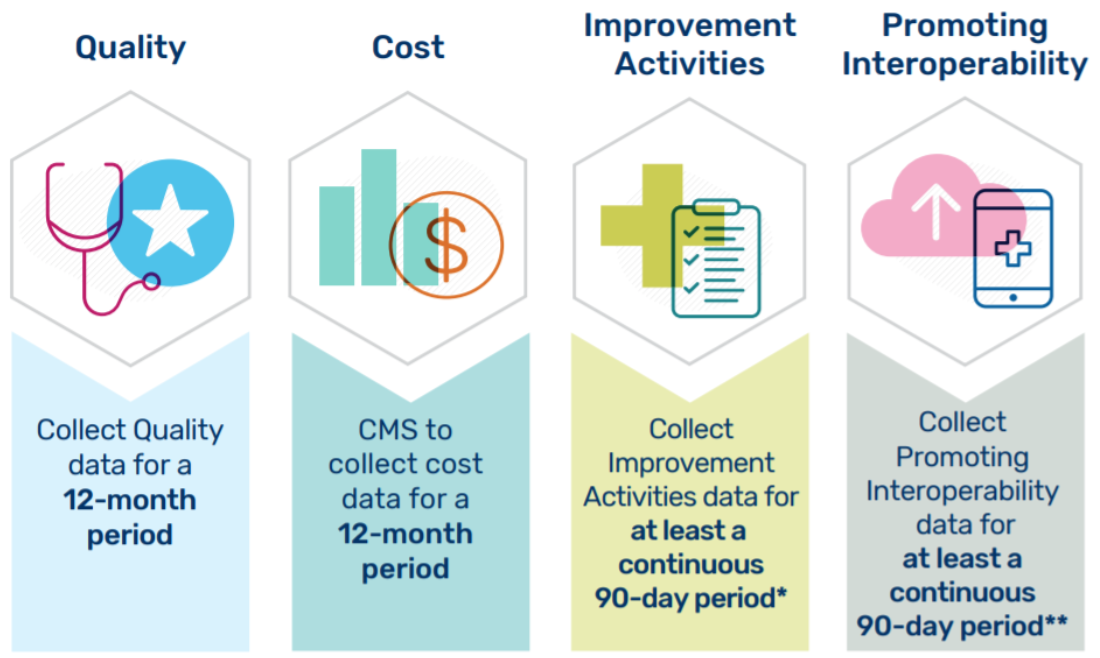
- Submit data for the entire 2018 calendar year.
- Submit data for at least a 90-day period within 2018 (only for the Promoting Interoperability and Improvement Activities categories) and a full calendar year for quality. Cost is also a full calendar year; however, no data submission is required.
- What about Promoting Interoperability (PI)?
- Did you apply for a 2018 PI hardship? If not, the window has already closed for applications.
- What edition EHR(s) are you using?
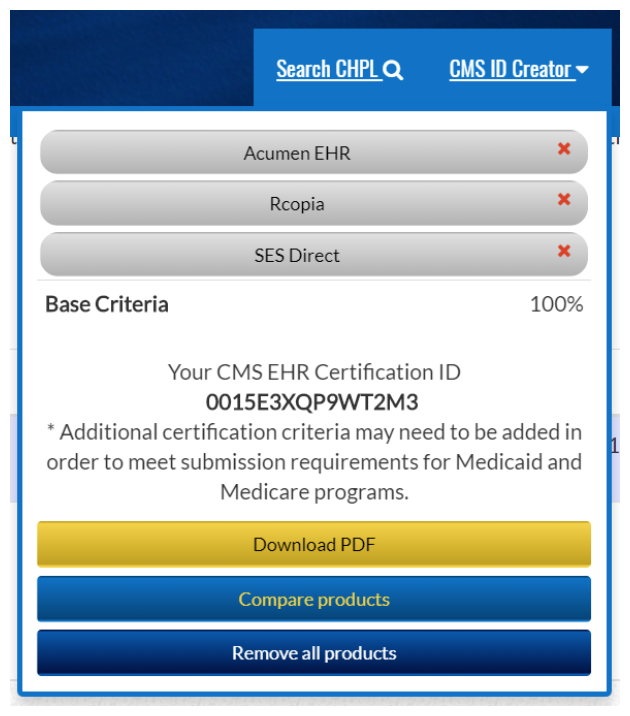
- Go to the ONC CHPL site to select all certified health IT vendors used during the 2018 period. This will generate your CEHRT ID.
- Acumen v8.0 customers who solely used Acumen for PI data will enter in the three following products:
- Acumen EHR v8.0 – 2015 edition
- SES Direct v2.0 – 2015 edition
- Rcopia v3 – 2015 edition
- What is your reporting period?
- Did you meet all the base measure requirements?
- What performance measures will you report?
- Are you eligible for any bonus points?
- Do you have a copy of your performance dashboard in case of an audit?
- Do you have supplemental documentation on file in case of an audit? (Hint: make sure to do a security risk analysis!)
- How will you submit your PI data?
- What about Improvement Activities?
- What activities did you select?
- Did your practice complete these activities for a minimum of 90-days?
- Do you have the correct documentation on file in case of an audit?
- How will you submit your improvement activity data?
- What about Quality?
- What quality measures did you select?
- Did you choose at least 6 measures (or a specialty set)?
- Take a look at the published benchmarks to decide which 6 are your most competitive.
- CMS will accept more than 6 measures and will score you on the top 6 measures.
- You must report on at least 50% of the patients that meet each measure’s population definition.
- Did you select at least 1 outcome measure?
- How will you submit your quality data?
- What about Cost?
- For Cost, there is no data to submit. Cost is calculated solely from administrative claims data.
Multiple pathways
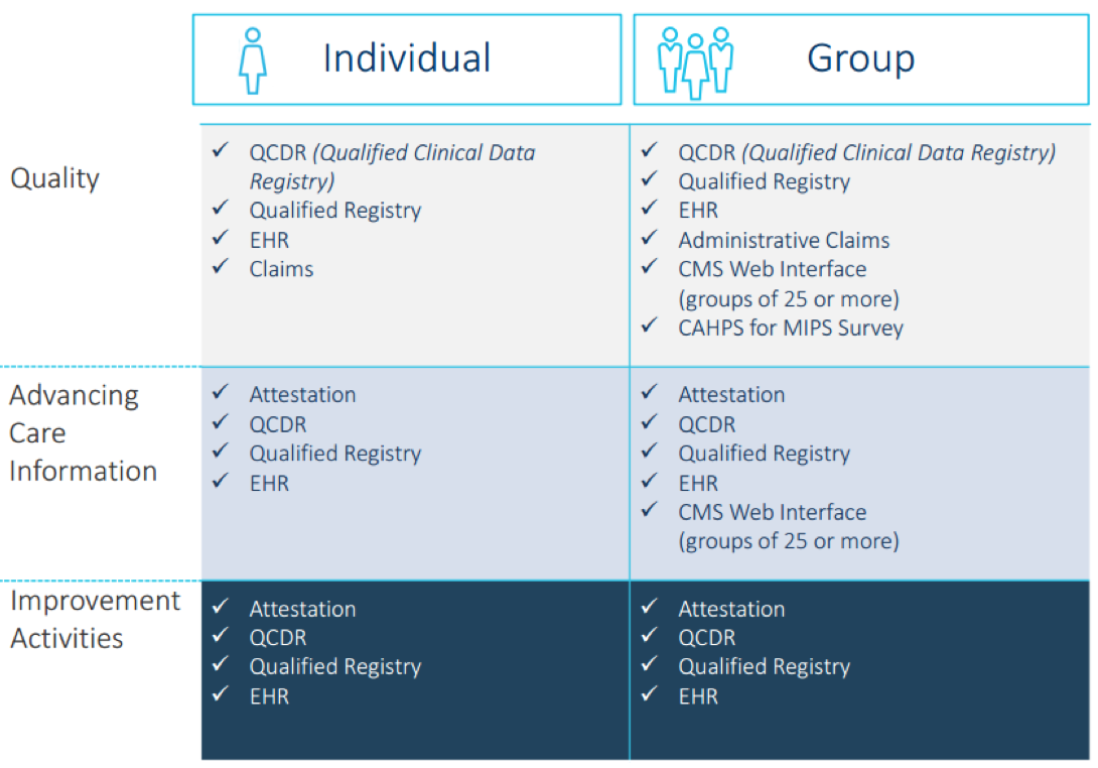
There are multiple pathways to submit your MIPS data to CMS. The submission mechanisms available to you depend on:
- Whether you are reporting as an individual or as a group
- The size of your group
- The type of health information technology you use
- The performance category on which you’re reporting
- Whether you participate in an MIPS APM or Advanced APM
To further complicate things, you do not need to choose the same data submission method for each category under MIPS!
Take a look at the image below. By now you should have a good idea on what method you will select under each category.
For most clinicians who are reporting without a third-party vendor, I am going to assume the majority will do the following:
- Quality: Submit data via the “EHR” option. This will typically include exporting a QRDA cat III XML (generated by your EHR) and uploading the file into the QPP submission website
- Promoting Interoperability:Manually attest via the QPP submission website
- Improvement activities:Manually attest via the QPP submission website
Disclaimer: Every situation is unique. You may be set up with a third-party tool (such as a Qualified Clinical Data Registry) or be part of a group/APM that will submit data on your behalf. It is extremely important to understand who is submitting data on your behalf, as well as when and how.
Set up your QPP account
To log in and submit data, clinicians will need to use the new HCQIS Authorization Roles and Profile (HARP) system. Previously, clinicians received their credentials through the Enterprise Identity Management (EIDM) system.
Returning clinicians: For all clinicians who previously had an EIDM account, you were automatically transitioned to HARP and will use your existing EIDM user ID and password to sign into the QPP website.
New clinicians: For all clinicians who didn’t have an EIDM account, you’ll need to enroll with HARP. For a step-by-step guide to signing up for a HARP account, refer to the QPP Access User Guide.
Don’t procrastinate here! Even if you are not ready to submit data, make sure you can log in.

Ready to submit?
So, you are ready to enter your data now, right? NOT SO FAST! One mistake I often see practices make is to forget to prepare an audit folder. CMS can request an audit up to 7 years after you submitted your data! If you don’t know what to have on file, take a peek at the PDFs found in this zip file. The file also contains a PDF on suggested documentation for improvement activities, which is very helpful.
OK, now you are ready!
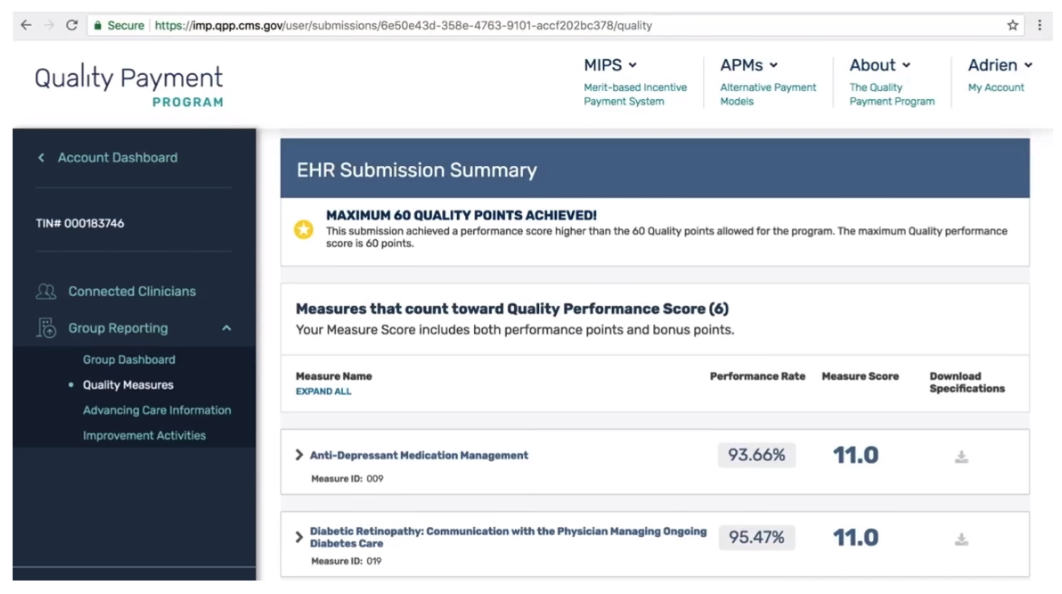
Now that you have all your information collected, you can log into the QPP site to submit data.
The QPP system is set up like a wizard in that it will walk you through each question one at a time to ensure you don’t miss a step.
The QPP system will score you in “real-time” so you understand how well you are doing in the program. It quantifies scores based on clinician submissions as data is being entered into the system. If you are submitting a quality measure without a benchmark, you will see the benchmarks change during the submission window as more clinicians submit data for that measure.
I highly encourage you to log into the QPP system early and often to familiarize yourself with the data submission and scoring method. You can update information as often as you like. CMS will use the last data update before the submission window closes.
Lastly, before you attest, take a minute to read this FAQ and watch this 38-minute YouTube video posted by CMS about data submission. Although the video is from last year, much of the content is still relevant.
Good luck!
Important MIPS Resources
• 2018 MIPS Data Submission Infographic
• 2018 MIPS Data Submission FAQ
• 2017 MIPS Data Submission YouTube Video
• QPP Helpdesk: 1-866-288-8292 or email qpp@cms.hhs.gov
 Diana Strubler, Policy and Standards Senior Manager, joined Acumen in 2010 as an EHR trainer then quickly moved into the role of certification and health IT standards subject matter expert. She has successfully led Acumen through three certifications while also guiding our company and customers through the world of Meaningful Use, ICD-10 and PQRS.
Diana Strubler, Policy and Standards Senior Manager, joined Acumen in 2010 as an EHR trainer then quickly moved into the role of certification and health IT standards subject matter expert. She has successfully led Acumen through three certifications while also guiding our company and customers through the world of Meaningful Use, ICD-10 and PQRS.




Leave a Reply