I am up in Seattle at the Annual Dialysis Conference where I had the opportunity to speak about meaningful use in the dialysis facility. We had a very engaging discussion, and during the Q & A it became clear there is still quite a bit of confusion surrounding the issue of dialysis patient encounters and their role in meaningful use. Those of you who understand the intricacies of this intersection can take a rain check on the blog this week and move on to bigger and better things.
Dialysis patient visits included in the 50% rule
At the heart of the matter is a fundamental requirement for participation in the CMS EHR Incentive Program. In an effort not to penalize primary care providers who see patients in multiple locations, some with EHRs and others without, ONC created what I have come to call the “50% Rule.” Simply stated, the 50% rule is asking if more than half of your face-to-face encounters during the reporting period occur in a venue (or venues) equipped with a certified EHR. The only physician encounters excluded from this calculation are hospital encounters using place-of-service codes 21 or 23 (Inpatient Hospital and Emergency Room-Hospital, respectively). The astute observer will note that every other POS code, including 65, ESRD Treatment Facility, is included. This is spelled out in question 168 (ID # 3065) on roughly page 81 of the CMS EHR Incentive Program FAQs. The inclusion of our dialysis encounters in the meaningful use calculus has also been confirmed by no less than three independent sources within CMS. For those who still do not believe the dialysis encounters are to be counted, I offer this direct quote from the questionnaire used during a meaningful use audit:
“If you utilize more than one office or other outpatient facility, could you please supply documentation which proves that 50% or more of your patient encounters during the EHR reporting period have been seen in offices or outpatient facilities where you utilize a CEHRT system?”
How does this impact the typical nephrologist? I have used the example below in many forums to explain it.
Calculating encounters for the 50% rule
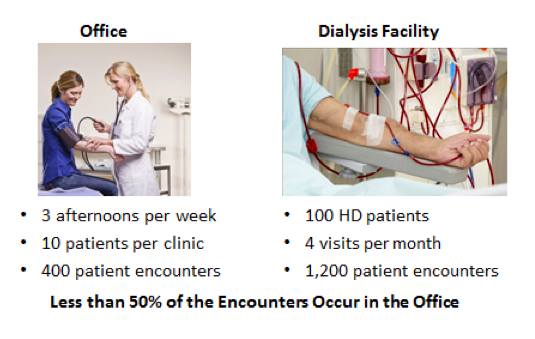
Suppose you are a solo doc and you divide your time between your office, the hospital and the dialysis facility. In this calculation, exclude all of your encounters in the hospital (unless you see patients in a hospital-based outpatient clinic, POS code 22). Basically you divide the face-to-face encounters you have in the office by the sum of those encounters plus the face-to-face encounters you have in the dialysis facility. If your fraction during the MU reporting period is less than ½ , as is the case in the example below, you have a couple of choices.
To use an office-based EHR in the dialysis facility or not to
During the first two years of the program (2011 & 2012) your choice in this circumstance was either to not participate in meaningful use (you were not eligible) or to utilize your office-based EHR to capture information about your dialysis patient encounters. Many nephrologists have opted for this second approach. They access their certified EHRs from the dialysis clinics and capture pertinent data like problem, medication and allergy lists. This option is possible because the Stage 1 hurdles are low, and it is attractive because the incentive is front-loaded, with most of the payments made in the first 2-3 years on the Medicare side of the program.
By accessing their CEHRT from within the dialysis facility, the eligible professional has fulfilled the eligibility requirement created by the “50% Rule.” Note this is not optional. If more than half of your encounters occur in the dialysis facility and you elected to report ONLY your office-based patient encounters when you attest for meaningful use, you are not in compliance with the program. If you receive an incentive in this setting, telling an auditor you did not understand the implication of this requirement is unlikely to result in a pat on the back.
Invoking a hardship exemption may be an answer
The flip side of the 50% Rule became apparent with the publication of the Meaningful Use Stage 2 final rule last fall. Starting this year, eligible professionals like nephrologists may invoke a 50% Rule related hardship exception, effectively opting out of the MU program. In our example above, there are again two options: 1) do not participate in the program or 2) access your certified EHR from within the dialysis facility. This second option in my view will become remarkably difficult for those who face the stage 2 objectives. The first option now has a new twist, one that I believe will impact a large number of nephrologists.
If, as in the example above, more than half of your encounters occur in a dialysis facility, and if the decision to deploy a certified EHR within the dialysis facility is outside of your direct control, you qualify for one of the new hardship exceptions. When you successfully file for a hardship exception, two things happen: you do not collect a meaningful use incentive (you did not demonstrate meaningful use) but, more importantly, you are excluded from the meaningful use penalty. For example if you file for the hardship exception this year, you will not face the 1% reduction in your Medicare Part B book of business for 2015.
Nephrologists may consider opting out of meaningful use in 2014
I think a few folks will take advantage of this unintended consequence this year, largely nephrologists who do not intend to obtain an EHR. Next year, however, I think we may see a larger interest in this exception as the early adopters (those who attested in either 2011 or 2012) face the Stage 2 objectives. They have put in their time, dragged their office-based EHRs into the dialysis facility, and often duplicated data entry in order to comply with the Stage 1 objectives. In 2014 they will face the daunting task of attempting to replicate this effort for the much tougher Stage 2 objectives, and if they are successful, they will receive a much smaller financial pay-off for their effort ($4,000 or $8,000 depending on which year they started).
Nephrologists represent roughly 1-2% of the professionals eligible for the meaningful use incentive in this country. The architects of the meaningful use framework almost certainly did not consider the impact the program would have on our specialty—specifically the challenges created by encounters in the dialysis facility or the access center. The confluence of tougher objectives and declining incentives may persuade a number of nephrologists to opt out of the program, an outcome that almost certainly qualifies as an unintended consequence. Would you consider opting out of meaningful use if the opportunity presented itself? Drop us a comment and join the conversation.




Jim Robertson says
Terry, I’ve read your posts in the past and remember you focusing on the “unique encounter” definition, concluding that all the visits in the dialysis center for one patient in the 3 month reporting period for first year Stage 1 meaningful use attestation would be considered a single “unique encounter.” Now it seems they’ll count as 12 unique encounters. Why the change?
Terry Ketchersid, Vice President and Medical Officer at HITSG says
Jim, you point out one of the most confusing aspects of the meaningful use framework within the realm of nephrology. I tend to think of this as a two step process. The first step requires looking at every outpatient encounter. This creates what I have referred to as the “50% rule”. In Stage 1 this was largely a determination of eligibility. If 50% of your outpatient encounters occured where CEHRT was deployed, you were eligible to participate in the meaningful use program. Once eligible, the majority of the MU objectives are counting “unique patient encounters”. This constitutes the second step and accounts for some of the confusion. The unique patient encounter creates the circumstance you describe, see the same patient 12 times during the reporting period and they are in the denominator for one of the MU objectives once. Stage 2 now introduces a hardship exception, which one could consider the other side of the 50% rule.
Gabe Rivera says
Hi
Got a wild scenario for you, we Nephrologists do not get paid to see dialysis patients in our offices unless the problem is not related to ESRD. Therefore CMS has forcefully identified ” clinic” for the dialysis patients, as the dialysis unit.
Now we have done 1600 encounters / 1600 total clinic encounters = 100%
Thanks
Gabe