 This week FMCNA Medical Officer, Rob Kossmann, emailed an interesting article from the BMJ Christmas issue, “Parachute use to prevent death and major trauma when jumping from an aircraft: randomized controlled trial.” The special BMJ Christmas issue invites articles with “originality” that may be research or non-research related. BMJ editorial staff encourage “lighthearted” and “novel” submissions noting that articles are subject to usual peer-review scrutiny.
This week FMCNA Medical Officer, Rob Kossmann, emailed an interesting article from the BMJ Christmas issue, “Parachute use to prevent death and major trauma when jumping from an aircraft: randomized controlled trial.” The special BMJ Christmas issue invites articles with “originality” that may be research or non-research related. BMJ editorial staff encourage “lighthearted” and “novel” submissions noting that articles are subject to usual peer-review scrutiny.
The parachute article came to my attention through email, but Terry Ketchersid pointed out that NPR reported on this article earlier in the week. As you might imagine, the title sparked widespread interest. During the NPR interview, the lead author explained the use of satire and humor to highlight “pitfalls of research” including the highly regarded randomized controlled trial (RCT) gold standard. The lesson of the parachute RCT is be diligent in examining research to make sure you understand the context and details of the study. It is of note (and totally awesome) that the article includes a citation for Sir Isaac Newton’s 1687 Law of Universal Gravitation.
Circumventing gravity
This is the catch, of course. We’ve all experienced the law of universal gravitation, so how can there be an RCT on parachute use? In fact, a 2003 BMJ article, “Parachute use to prevent death and major trauma related to gravitational challenge: systematic review of randomised controlled trials,” confirmed that no RCTs regarding parachute use exist, suggesting that, “Individuals who insist that all interventions need to be validated by a randomised controlled trial need to come down to earth with a bump.”
The 2018 parachute RCT authors report on 23 friends and family who were randomized to jump from an aircraft with a parachute as part of the intervention group or with an empty back pack as part of the control group. Randomization is described in detail and the intervention and control group characteristics are listed in a table including history of broken bones, acrophobia, parachute use, and family history of parachute use. Data was collected at the time of the jump and in follow up 30 days post jump. Outcomes of interest included death and major traumatic injury as measured by the validated Injury Severity Score. Proper statistical analysis was performed with the conclusion that there was no significant difference in outcomes for the intervention versus the control group.
Here is the “minor caveat” for the study: The lower than expected incidence of death and major trauma in the intervention and control groups is likely secondary to participants jumping from the aircraft from an average altitude of 0.6 m on aircraft moving at an average of 0 km/h. Randomized participants jumped from either a stationary airplane in Katama Airfield in Martha’s Vineyard, MA, or from a helicopter at the Yankee Air Museum in Belleville, MI. Among the study limitations: “First and most importantly, our findings might not be generalizable to the use of parachutes in aircraft traveling at a higher altitude or velocity.”
The authors propose that “…critics might further argue that although randomized controlled trials are the gold standard for evaluating treatments, their results are not always guaranteed to be relevant for clinicians. It will be up to the reader to determine the relevance of these findings in the real world.” Even RCTs have limitations and the interpretation of results and data requires diligence, a “complete and critical appraisal of the study.”
Life is more than RCTs
Some of my key takeaways:
- Seriously, it is good not to take medicine so seriously all the time
- Seriously, maybe we perseverate over details that aren’t always the most beneficial for patients
- Seriously, maintaining equipoise* is difficult and complex
- Seriously, how much of patient care is about RCTs?
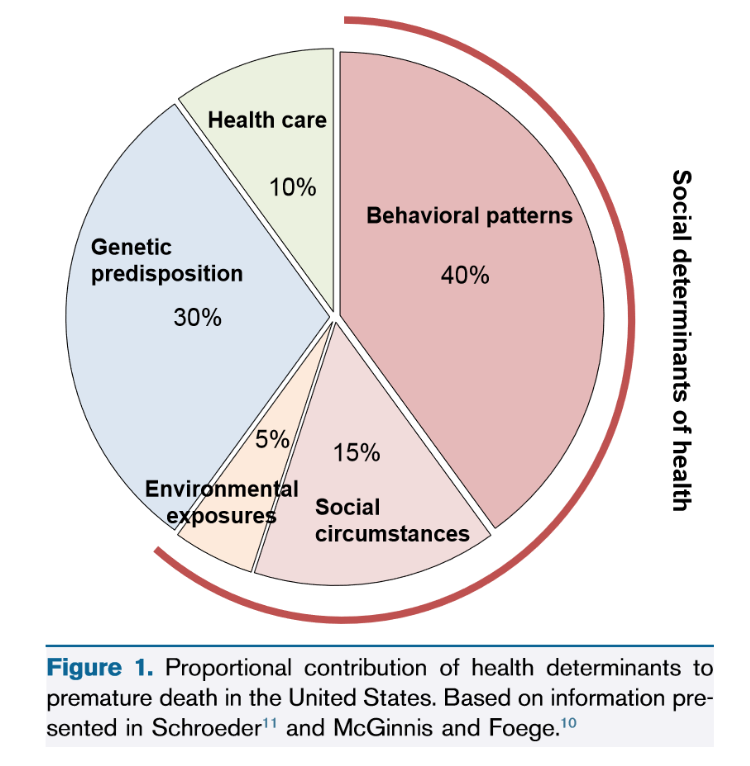
While research rigor relies on RCTs and such studies provide valuable safety and efficacy data, good patient outcomes may not hinge on research insights alone. In 2007, a NEJM article on health outcomes in the U.S. reported that medical care plays a small role in preventing premature death. In March 2018 a comprehensive AJKD article described the impact of social determinants of health (SDOH) on outcomes in CKD. Dr. Hall, the article author, notes that race, ethnicity, socioeconomic status, health insurance, and residential neighborhoods create disparity in the incidence, progression, and treatment of CKD. These social conditions “…govern access to resources that influence health and disease.”
Dr. Hall suggests that pragmatic clinical trials are needed to include vulnerable patient populations who may be excluded from traditional RCTs. Pragmatic clinical trials occurring in typical health care settings may identify interventions that work in certain geographies with the use of new tools such as telehealth technologies.
Let’s dance
My mother is receiving in-home end-of-life care. Every week I touch base with the hospice nurse and we review her skin care, pain management, blood pressure, and arm circumference all of which are pertinent to her care. Months ago hospice suggested that she might enjoy listening to music for relaxation. My sisters and I have assembled a CD collection of her favorite musicals: Sound of Music, Oklahoma, Fiddler on the Roof, and West Side Story. We heard all of these LPs and watched these movies many times during childhood because she loved them so much. Over the holiday while visiting we spent several hours singing and dancing to the hits….Oklahoma, where the wind comes sweepin’ down the plain, and the wavin’ wheat can sure smell sweet when the wind comes right behind the rain. She smiled for us, and I’m sure this was good therapy.
The parachute RCT is an important reminder of the shortcomings of the RCT gold standard. Take them seriously for what they actually show for the population studied in the circumstance created. Consider the benefits of pragmatic studies that define meaningful interventions for diverse patients in personal situations of geography and socioeconomic status. Seriously, don’t be too serious and miss the impact of human behavior and musical joy.
Wishing you humor, practicality, and music for a Happy New Year!
 Dugan Maddux, MD, FACP, is the Vice President for CKD Initiatives for FMC-NA. Before her foray into the business side of medicine, Dr. Maddux spent 18 years practicing nephrology in Danville, Virginia. During this time, she and her husband, Dr. Frank Maddux, developed a nephrology-focused Electronic Health Record. She and Frank also developed Voice Expeditions, which features the Nephrology Oral History project, a collection of interviews of the early dialysis pioneers.
Dugan Maddux, MD, FACP, is the Vice President for CKD Initiatives for FMC-NA. Before her foray into the business side of medicine, Dr. Maddux spent 18 years practicing nephrology in Danville, Virginia. During this time, she and her husband, Dr. Frank Maddux, developed a nephrology-focused Electronic Health Record. She and Frank also developed Voice Expeditions, which features the Nephrology Oral History project, a collection of interviews of the early dialysis pioneers.
Image from www.canstockimage.com
*You may know all about clinical equipoise, but I had to look it up. Clinical equipoise means that the researchers begin the study believing that the intervention to be studied may or may not be better than current care. An ethical dilemma is created when investigators prematurely believe that the treatment intervention is better for at least some potential treatment subjects. This creates the possibility that some subgroups of patients will not be studied because investigators do not want to prevent them from getting treatment. This may skew the population that is ultimately studied. The parachute RCT authors note that previously RCTs on parachute use may not have been undertaken due to pre-existing beliefs about the benefits of parachutes: “Lack of equipoise could inhibit recruitment of participants in such a trial. However, whether pre-existing beliefs about the efficacy of parachutes would, in fact, impair the enrollment of participants in a clinical trial has not been formally evaluated.” 😊



Glenn Pearl says
Dear Dr. Maddux,
With much delight and interest, I have been listening to various interviews conducted as a part of the Oral History of Nephrology. I am an ESRD patient, currently with transplant, and started on dialysis in 1976 when I was 14 years old. I dialyzed in a pediatric unit at Albert Einstein in the Bronx, under Dr. Ira Greifer.
I am contacting you because I am doing research project.
I would like to send an e-mail along with more specifics. Would you be able to e-mail me, so that I may send along more detailed information? Thank you, Glenn Pearl