During each of the last four years we have operated a very successful CMS-qualified PQRS Registry. Participation in this process has created some very interesting opportunities for us. Historically we have focused on “renal facing” measures and measures groups. In our experience reporting the CKD measures group (CKD MG) using the 30-patient sample method has been the most popular choice among our customer base.
Each year CMS manages to make a few minor tweaks in the PQRS program and 2012 is no different. Today let’s review what they have in store for you with regards to the CKD MG.
Changes to PQRS that affect nephrologists
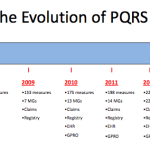
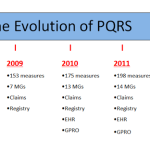
The first thing veterans of the PQRS program will notice is the measures within the CKD MG have changed. The 2012 version contains the following four individual PQRS measures:
- # 110 Preventive Care and Screening: Influenza Immunization
- # 121 Adult Kidney Disease: Laboratory Testing (Lipid Profile)
- # 122 Adult Kidney Disease: Blood Pressure Management
- # 123 Adult Kidney Disease: Patients on Erythropoiesis-Stimulating Agents (ESA)—Hemoglobin Level > 12.0 g/dL
Globally, the CKD MG denominator has expanded and now includes Stage 3 patients as well as those with Stage 4 or 5. This will actually help those of you who had difficulty last year identifying 30 unique Medicare Part B FFS patients with either Stage 4 or 5 CKD. The accompanying CPT codes have not changed. The patients you are expected to report on are patients you either saw in the office, a nursing home or in their home.
Beyond the global changes, each of the four measures above has changed slightly:
110 Influenza Immunization
The renal-related immunization measures were all retired last year and this general preventive care measure has taken their place. When included in the CKD MG, measure 110 applies only to patients 18 years of age and older who encountered the physician between January and March OR October and December. Stated another way, if the adult stage 3, 4 or 5 CKD patient sees you outside the flu season (between April and September) measure 110 is not applicable and this patient will not impact your reporting or performance rate for measure 110.
121 Lab Testing (Lipid Profile)
As the name implies, 121 has been streamlined to look specifically at whether or not a lipid profile has been performed for this patient within the past 12 months. The renal-related lab tests (calcium, phosphorus and PTH) have been dropped from this measure for 2012.
122 Blood Pressure Management
Just when you thought it was safe to go back into the water, the BP management measure brings an interesting twist this year. This measure is specifically looking for adult stage 3, 4 or 5 CKD patients WITH documented proteinuria. The PQRS measure specifications define proteinuria as “> 300 mg of albumin in the urine per 24 hours OR albumin creatinine ratio (ACR) > 300 mcg/mg creatinine OR protein to creatinine ratio > 0.3 mg/mg creatinine.” The MG specs go on to state “Measure #122 need only be reported when the patient also has the following diagnosis code indicating Proteinuria: 791.0.” My interpretation is look for either the ICD-9 code (good luck with that) or laboratory evidence of proteinuria to determine whether or not to report 122 for your CKD patients. The numerator for this measure has not changed for 2012.
123 Patients on ESA—Hemoglobin Level > 12.0 g/dL
New for 123 is the fact that taking an ESA is a requirement to be counted in this measure. That’s not clear from the measure specs, but it is clear from the exercise all qualified registries were required to participate in. Further, although the CKD MG denominator includes Stage 3 CKD patients, measure 123 does not. Effectively this suggests one would report 123 only for adult Stage 4 or 5 patients receiving an ESA.
Pitfalls that require further clarity
In years past when CMS combined individual measures to create a MG they typically created a common denominator, even in circumstances where the denominators differed when the measures were reported individually. This created a scenario in which the provider was answering several quality measures for the same patient(s). This approach appeals to the logical intuition most of us posses. Oddly things appear to be different this year. The numerators for the CKD MG measures are reasonably clear, but be careful as you examine the denominators.
Remember, as was the case in 2011, measures groups containing a measure with a 0% performance rate will not be counted as satisfactorily reporting the MG. If you are reporting the 30-patient sample method for the CKD MG and only a handful of your 30 patients have proteinuria, at least one of those proteinuric patients must have either a controlled BP or they must have an action plan in place. If not, your performance rate for 122 is zero and you will not receive credit for reporting the CKD MG.
Reporting the CKD MG has been an attractive choice for nephrologists in the past and I think with some work that can continue in the future. We will continue to work to clarify some of the outstanding issues above. In the meantime join the conversation and share your experience with us.
[polldaddy poll=6284451]

Maureen Gallo says
The article was fine but your registry is still not up and running and our MDs are anxious to begin. We were intially told this would be available to us in August, now are told it will be ready some time in September.
We will begin by creating our own forms and the MDs can go ahead and start.
Maureen
Terry Ketchersid, Vice President and Medical Officer at HITSG says
We are pedalling fast Maureen! I have asked one of our PQRS specialists to contact you as I beleive we can improve the experience for you.