During my internal medicine residency at the University of North Carolina (UNC) it was not uncommon to cross paths with Dr. Carl Gottschalk. My recollection of the Kenan Professor of Medicine is of a distinguished bespectacled gray-haired gentleman with a purposeful stride. Even before my nephrology fellowship I knew about Dr. Gottschalk’s role in chairing the 1967 group that published the “Report of the Committee on Chronic Kidney Disease,” the Gottschalk Report, which established dialysis and renal transplant as valid treatments and recommended Medicare entitlement for patients requiring this treatment.
Dr. Gottschalk graduated from the University of Virginia Medical School in 1945. He interned at Mass General and came to UNC in the early 1950s as a cardiology fellow, but his research centered on renal physiology, with a lab well known for renal tubule micro-puncture. As a renal fellow I discovered that Dr. Gottschalk pioneered the strong renal physiology faculty at UNC.
Nephrology fellowship: Real life and real people
Early in my medical school clinical years, I knew I preferred the physical diagnosis and problem-solving nature of internal medicine. As an internal medicine resident I admired the nephrology fellows and attendings who cared for the acute, gravely ill ICU/CCU/SICU patients and the complex, chronically ill 3 West nephrology service patients. In my resident’s view, the nephrologists were some of the smartest people in the hospital.
In 1987 Dr. Bill Blythe, Chief of the Division of Nephrology, gave me the opportunity to be a renal fellow. The Big Bang of my nephrology universe includes many formative lessons:
- Patient-centered care from Dr. Blythe (well before it was the hot thing),
- Intellectual and precise clinical assessment from Ron Falk,
- Physical diagnosis and chronic management from Kathy Huffman,
- Chronic dialysis from Bill Mattern,
- Renal transplant from Bill Finn,
- Renal physiology from Arthur Finn and Bill Lassiter, and
- Renal pathology and softball from Charles Jennette.
Intermingled with the elements of my nephrology knowledge, Dr. Blythe and many others coalesced my medical training around real life and people. Dr. Blythe died in 2000, but the William Blythe Essay Competition is held every year to honor his love of literature and writing. Dr. Blythe wove literature, life, ethics, and philosophy into his everyday teaching rounds; on Saturday morning rounds this included homemade bread and jam shared around the table as patient cases were presented. A favorite Blythe lesson of mine is a story he told at our annual internal medicine “Pearl Day” when selected attendings gave lectures on topics of their choice. The story went something like this: A typical rounding team was gathered in the hospital corridor while a medical school student presented the findings for a new admission. The student produced a prodigious amount of data including the following blood work lab data:
- Potassium = 5.5meq/L
- Calcium = 13.6 mg/dl
- Glucose = 64 mg/dl
- BUN = 800 mg/dl
- Total protein = 2.4 mg/dl
- Phosphorus = 4.1 mg/dl
- Sodium = 284 meq/L
The younger physicians on the team commenced with an animated discussion of possible diagnoses centered on hypercalcemia and the certain serum sodium error. All agreed that this patient was quite ill and most likely to have a poor prognosis. After much discussion the senior physician (by description a nephrologist remarkably similar to Dr. Blythe) calmly suggested a foray to the patient’s bedside. The team headed to the patient’s room and, led by the wise mentor, discovered a perfectly healthy shark.
Each day I think about the reams of data that trigger action and intervention by physicians. Nephrologists are managing data input and output from practice EHRs, hospital systems, and a third major entity, the dialysis clinical system. Organization and review of this data can be complicated and time consuming, perhaps not even humanly possible. At the end of the day data management must be correlated with physical patient assessment or we risk the misdiagnosis of the healthy shark.
A shortage of nephrology fellows
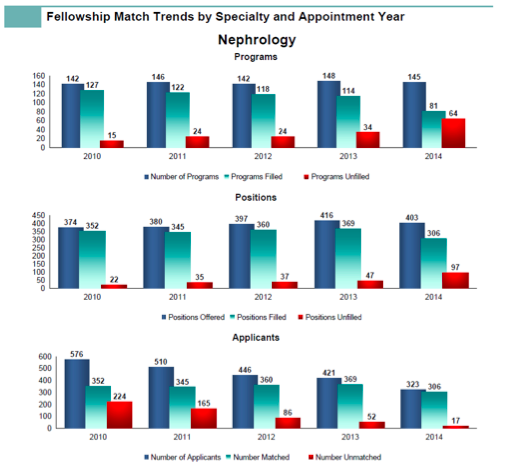
Recent nephrology fellowship information has made me wonder if burgeoning nephrology data, chronic care, multiple care venues, and data distraction have darkened the nephrology patient doorways for young physicians. Recently the National Resident Matching Program (NRMP) published the results of the 2013-2014 specialty matching service.
- 3,552 U.S. fellowship programs in 55 specialties offered 8,242 fellowship positions.
- In this match there were 323 applicants for 403 nephrology fellowship positions.
- Only 76% of nephrology fellowship positions were filled.
- Out of 13 internal medicine fellowship specialties only Geriatrics fared worse than nephrology.
The percentage of filled nephrology fellowship positions has been decreasing since 2010 despite a decrease in the overall number of nephrology fellowship positions offered. In 2010 there were 576 total nephrology fellowship applicants compared to 323 applicants in 2014. Overall there are 45 fewer nephrology fellows in 2014 compared to 2010.
Balancing data and patient care
USRDS data in recent years has shown overall growth of prevalent dialysis patients, not because more new patients are starting dialysis, but because more patients on dialysis are living longer. In tandem with this dialysis work, nephrologists and other providers are making improvements in diabetes, hypertension, and cardiovascular disease management; in CKD screening; and in interventions to slow progression to ESRD.
Quality and outcomes data should support this improvement in patient outcomes, but not become the focus of our nephrology practice. Hopefully young physicians will find nephrology mentors, philosophers, and leaders to lure them to nephrology fellowships. If not, nephrology may soon have to pioneer high-tech solutions for a virtual bedside presence.
Are you feeling the person power shortage in your practice? How is your work-life balance with data and patient care? Will nephrology supply and demand be an issue and, if so, what do you think is causing it? Post a comment and let us know what you think.



Leave a Reply