I know it is hard to believe, but the first month of 2013 is behind us and February is well underway. Last week we witnessed the excitement of the Super Bowl, a blow out in the first half, a blackout to start the second half, followed by a finish that rivaled the half-time show in entertainment value. Last week also saw the arrival of a much-anticipated announcement from CMS.
Last year many nephrologists experienced the market churn created by Accountable Care Organizations (ACOs). Health systems, primary care providers and a wide range of other health care providers debated, studied and anxiously faced the pressure of determining whether or not they should join a local ACO. In the background, a group of prominent stakeholders within the renal community were making the case that the ESRD patient population was not a good fit with the classic ACO or medical home model. How could CMS expect a primary care provider to the lead the team providing care to this complex patient population? Out of this emerged the concept of a “Renal ACO”, an idea that envisioned nephrologists and dialysis facilities working closely together to provide better coordination of the care delivered to this group of patients.
On February 4, CMS made it official. The Center for Medicare and Medicaid Innovation published a request for application for the development of what it is calling ESRD Seamless Care Organizations (ESCOs). The stated goal of these organizations is to “improve outcomes for Medicare beneficiaries with ESRD and reduce total per capita expenditures by creating financial incentives for dialysis facilities, nephrologists, and other Medicare providers of services and suppliers to collaboratively and comprehensively address the extensive needs of the complex ESRD beneficiary population.” I know that’s a mouth full. I have emphasized the word “total” to highlight the fact that the cost bucket under examination is not simply the Medicare Part B component of patient care most of us are familiar with, but it also includes Part A (largely hospital care) and Part D (medications).
CMS anticipates awarding 10-15 ESCO contracts and they are in a hurry, expecting to see letters of intent by the Ides of March, submission of actual applications by May 1, 2013, and the programs up and running by the fourth quarter of this year. Each ESCO must contain a dialysis organization(s), a nephrologist(s), and at least one other Medicare provider or supplier. This is graphically depicted in figure 1 from the RFA displayed below.
ESCO Compositional Structure
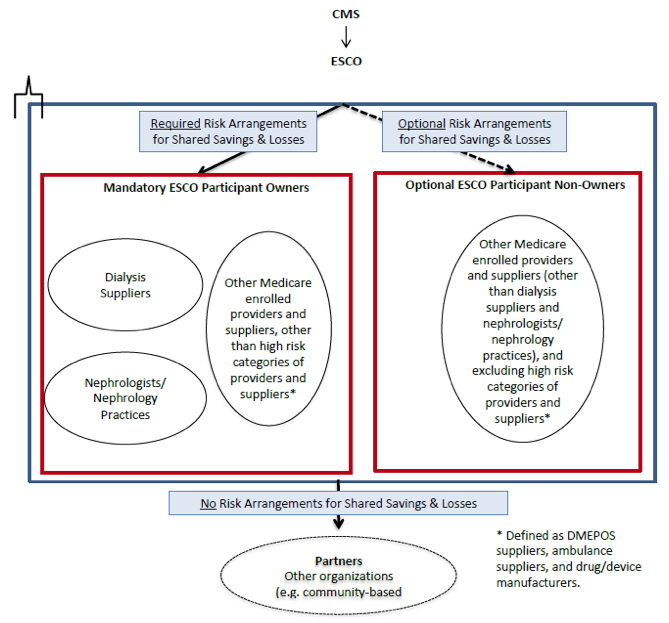
The ESCOs must have a minimum of 500 ESRD patients, with patient attribution occurring through a defined process. If the dialysis organization is considered a large dialysis organization (LDO), the ESCO may only contain a single dialysis organization. The program defines an LDO as a dialysis organization with more than 200 dialysis facilities. ESCOs that involve an LDO must take “2-sided risk” out of the gate. This amounts to true performance risk in that the ESCO shares savings garnered through coordinated care with CMS, but if savings does not occur (the patients under the care of the ESCO consume more Medicare dollars than targeted), the ESCO is on the hook financially. ACOs created without the involvement of an LDO have the opportunity to ease into the 2-sided risk model. The programs have three-year time frames and there are caps on upside and downside risk as well as protections from catastrophic claims.
Last week was indeed exciting. Now that the Super Bowl has concluded and those multi-million dollar commercials are being replayed on YouTube, we can turn our attention where it belongs—March Madness is but a few short weeks away. Keep your ears open; we will certainly hear more about ESCOs in the coming weeks as a number of very intelligent folks within the renal community sharpen their pencils and slog through the details of this important program. Make no mistake about it, however; ESCOs will likely join the rapidly approaching Physician Value-Based Payment Modifier as forces that shift focus away from business as usual in the day-to-day lives of nephrologists.



Leave a Reply